Acquired bilateral nevus of Ota-like macules
“Acquired bilateral nevus of Ota-like macules,” another medical term that may sound complicated at first glance. Its name is derived from the English translation of Acquired bilateral nevus of Ota-like macules (ABNOM).
As the name suggests, it bears some similarity to nevus of Ota. This skin problem has different names circulating online, such as “brown-blue cheek moles,” and “cheek or jagged moles.” In English, it is also called Hori’s macules. It is clear that there is no unified name for this skin problem, and for the purposes of this article, it will be referred to as ABNOM.
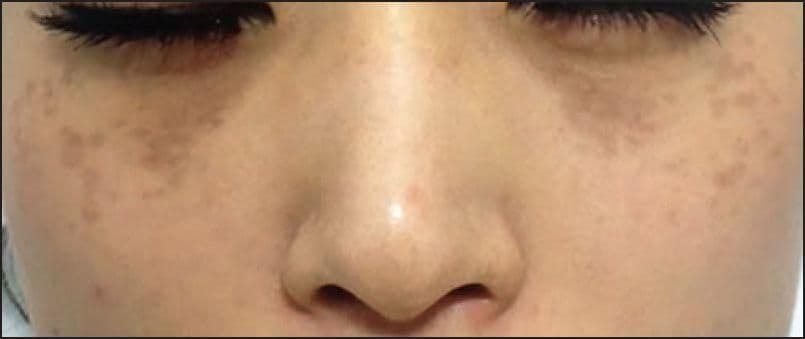
There is no official statistic on the incidence rate of ABNOM in Hong Kong, but the incidence rate among Asians is 0.8%. It seems to be a relatively uncommon issue that predominantly affects women, with a female-to-male ratio of six to one. ABNOM generally begins to appear around the ages of 20-30, and in some cases, it may be due to a family history of the condition. The clinical symptoms include blue-black, brown, or gray patches that appear symmetrically on both sides of the forehead, upper and lower eyelids, and cheekbones. Some patients, and even doctors, may confuse ABNOM with freckles, hormonal spots, or other skin issues that commonly appear in the same areas.
The formation of ABNOM is believed to be caused by melanocytes, or pigment-producing cells, entering the dermis for unknown reasons and becoming quiescent (melanocytes are not supposed to exist in the dermis). These cells then become activated due to factors such as UV radiation, hormones, or skin inflammation, releasing melanin and forming ABNOM. It is unknown why this phenomenon only occurs in specific locations.
Because ABNOM is a dermal problem, its treatment can be more complex than other pigmentation issues. The melanocytes in ABNOM are concentrated near blood vessels, and hormonal spots often appear at the same time, increasing the likelihood of side effects after treatment. Accurate diagnosis is crucial since the prognosis and treatment approach may differ depending on the case. Some doctors may try to treat ABNOM with fruit acids, diamond peels, or depigmenting agents, but the results are often unsatisfactory. Currently, the most effective method is using nanosecond laser therapy. Doctors will choose lasers with wavelengths of 694nm, 755nm, or 1064nm. The 1064nm laser can penetrate deeper into the skin, resulting in more significant improvements. Multiple treatments spaced one to three months apart are usually necessary to achieve optimal results.
Side effects of treatment may include post-inflammatory erythema, post-inflammatory hyperpigmentation, and post-inflammatory hypopigmentation. Treatment for ABNOM can be more complicated, so it is essential to consult with a doctor before undergoing treatment.